Bone diseases of the Jaws
1. Pseudo-diseases: a. Bone marrow defect, b. Osteosclerosis, c. Submandibular salivary gland defect.a. Bone marrow defect: a variant of normal but is mistakenly diagnosed as abnormal.There are usually no clinical signs nor symptoms. No treatment required.b. Osteosclerosis: an area of dense bone within the jaw. There are usually no clinical signs nor symptoms. No treatment required.c. Submandibular salivary gland defect: a developmental abnormality that appears as a radiolucent area in the mandible. There are usually no clinical signs nor symptoms. No treatment required.
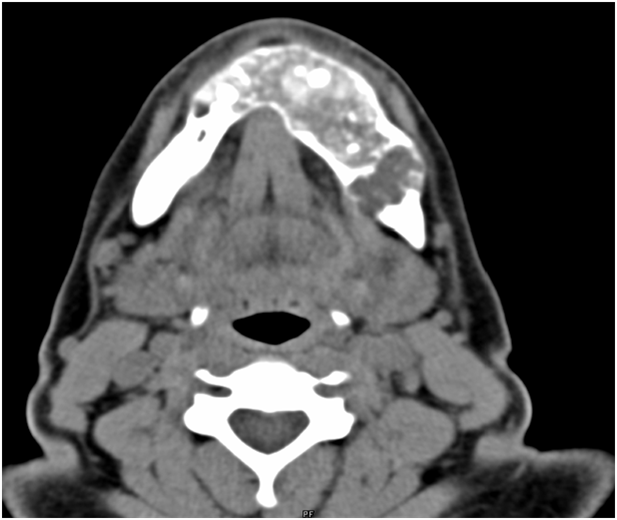
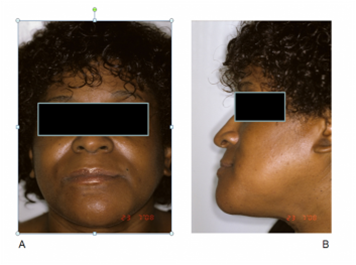
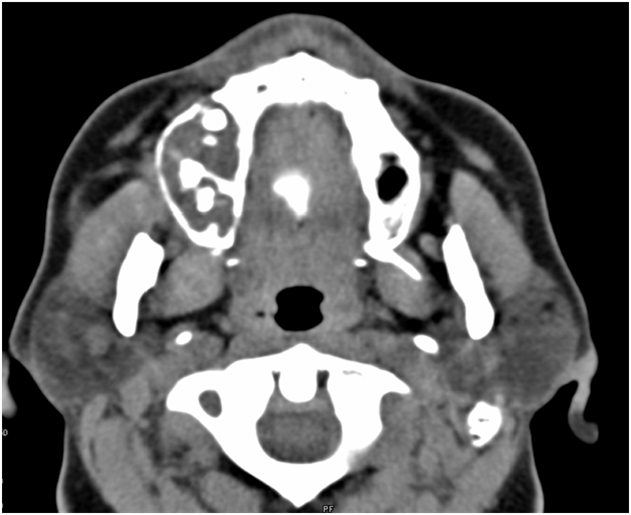
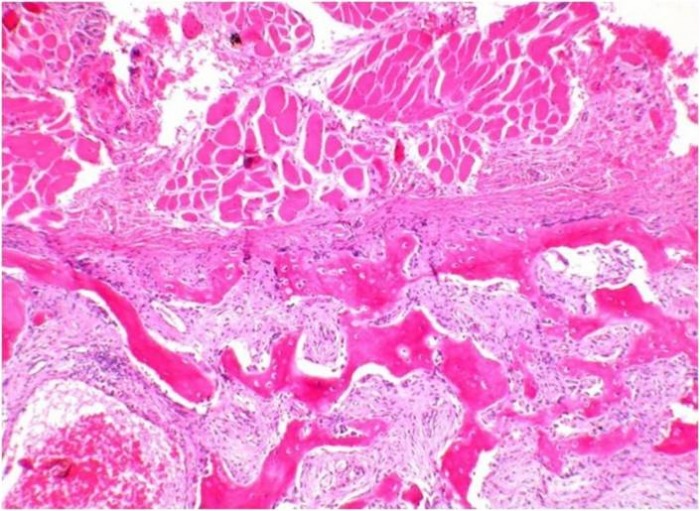
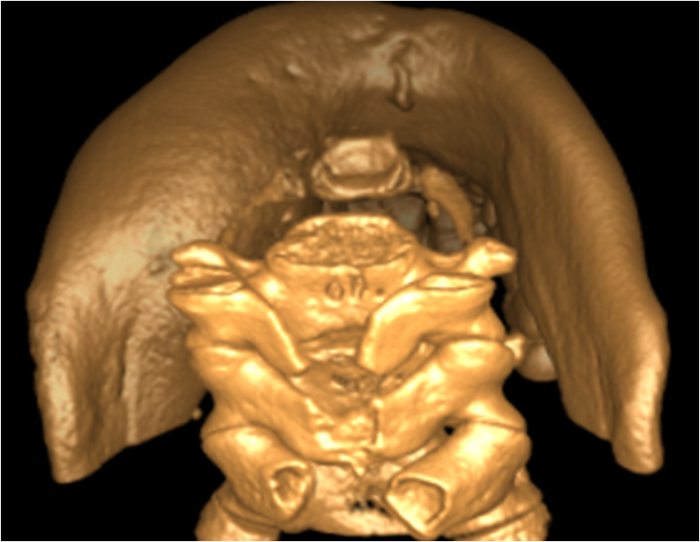
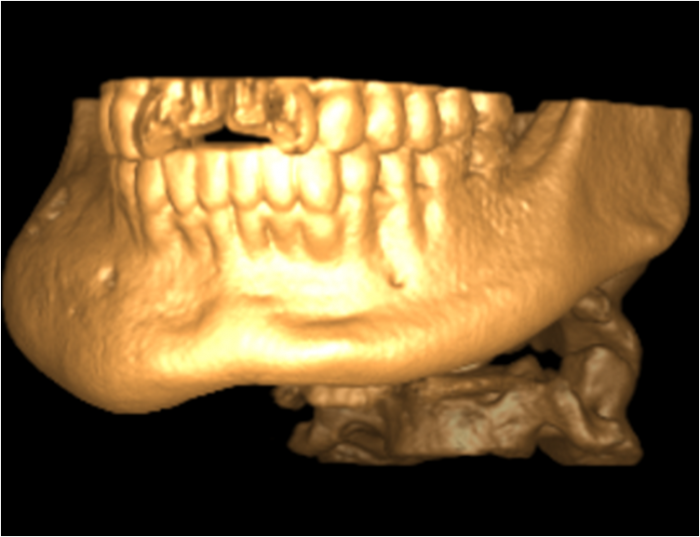
2. Non-neoplastic diseases of bone: a. Osteogenesis imperfect, b. Osteopetrosis, c. Paget disease of bone, d. Fibrous dysplasia, e. Cherubism, f. Cemento-Osseous Dysplasias, g. Aneurysmal Bone Cyst. a. Osteogenesis imperfect :an inherited disease of the skeleton and other connective tissues caused by mutations in the genes. Collagen is the main component of bone matrix, dentin, tendons, ligaments and the sclera. The dental condition known as dentinogenesis imperfecta is often inherited with osteogenesis imperfecta. There is no cure for this disease.b. Osteopetrosis: an inherited disease of bone in which there is failure of normal osteoclastic resorption. The imbalance between osteoblastic apposition of bone and osteoclastic resorption leads to increasing bone density throughout the skeleton. Bones exhibit a homogenous, fine grain density throughout the skeleton. There was no treatment for this disease because there was no way to stimulate the patient’s own osteoclasts to resorb bone.c. Paget disease of bone: skeletal disease of unknown cause. Abnormal resorption and deposition of bone. May involve many bones. Osteoclastic activity creates bone cavities, later, new bone is deposited in an abnormal pattern (cotton wool appearance). The disease may burn-out leaving enlarged and dense bone comprised of atypical trabeculae of Paget bone. It is uncommon for Paget disease to occur before age 40. Mild cases are asymptomatic and require no treatment. Pain may be controlled with aspirin or indomethacin. Steroids have been reported to suppress the disease but require large doses with the risk of Cushinoid syndrome. d. Fibrous dysplasia :group of lesions in which normal bone is replaced initially by fibrous connective tissue. Over time, the lesion is infiltrated by osteoid and cementoid tissue. Normal trabeculae of bone undergo osteoclastic resorption to make room for the expanding cellular mass. New bone is formed within the cellular mass. Purely radiolucent forms have been described, but the most common appearance is that of a finely trabeculated radiodensity, the so called “ground glass” appearance. Fibrous dysplasia is non-hereditary Caused by a mutation in a somatic cell. Surgery is the only treatment.e. Cherubism: rare, inherited disease causes bilateral enlargement of the jaws. The disease has little in common with fibrous dysplasia of the jaws. The disease occurs mainly in the mandible, but may also involve the maxilla. Usually develops at 2-6 years of age. Cherubism appears as radiolucent and multilocular lesions. The radiographic features are virtually pathognomonic. Expands cortices of the mandible, teeth are displaced anteriorly as lesionsexpand. The lesions may stop growing and regress during the teens but cosmetic recontouring recommended for esthetics. f. Cemento-Osseous Dysplasias:includes,1- Periapical Cemental Dysplasia.2- Florid cemento-osseous dysplasia. 3- Focal Cemento-osseous dysplasia. All of these lesions represent the same histopathological process, but are distinguished by the location and extent of lesions in the jaws. PCD is a localized change in bone metabolism. It occurs at the apices of lower anterior teeth.FCOD has Same histopathology as PCD, Called FCOD when lesions are present in three or more quadrants. Uncomplicated osseous dysplasia requires no treatment. teeth should not be extracted without good reason. Traumatic ulceration of overlying mucosa also predisposes to infection. Denture fit should be carefully monitored to avoid this. In those cases with superimposed infection, sequestrectomy with primary closure and antibiotics are the accepted treatment.g. Aneurysmal Bone Cyst: A reactive lesion of bone rather than cyst or neoplasm. Resembles CGCG due to the histologic presence of giant cells. Occurs in individuals less than 30 yrs, mostly females. Rapid swelling due to expansion of bone. Painful. Surgical treatment is recommended.
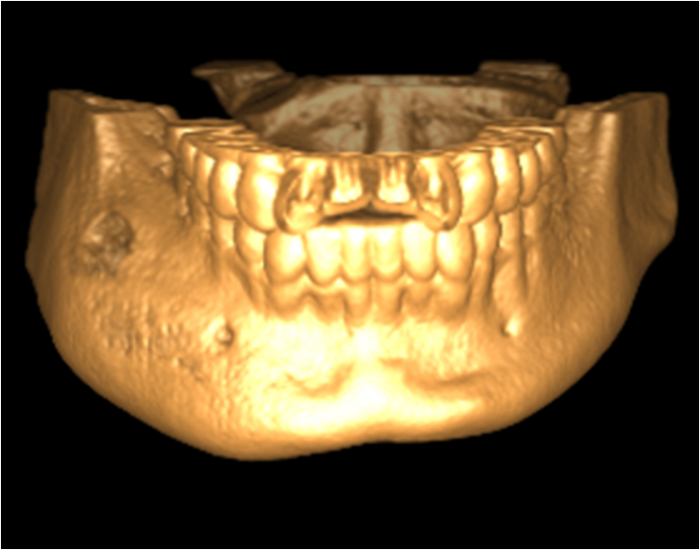
3. Bone tumor: a. Central giant cell granuloma, b. Ossifying and cementifying fibroma, c. Langerhans Cell Histiocytosis.a. Central giant cell granuloma: controversial lesion arising centrally within bone. Presents as a painless swelling on routine examination. Seen in 2 or 3rd decade. The middle and anterior segments of the jaws are most frequently involved, seldom are these lesions found posterior to the first molar area. The lesion is purely radiolucent. It may be unilocular or multilocular with classic soap bubble appearance. Adjacent teeth may be resorbed or moved bodily. Although large tumors cause jaw expansion, it is uncommon for the tumor to penetrate the cortex. b. Ossifying and cementifying fibroma: This is a benign tumor arising centrally withinbone. Also considered a type of fibro-osseous lesion. It is composed of fibroblasts sometimes exhibiting a compact, whirled appearance with variable amounts of collagen between tumor cells. Can occur in any decade, but most common in young adults. Most common in the mandible, Inferior to the premolars and superior to the mandibular canal. In maxilla commonly appears in the canine fossa or the zygomatic process of the maxilla. Those tumors with little calcified material are radiolucent. Those with much calcified matrix are radiodense. Intermediate degrees of radiolucency-radiodensity may be seen. The treatment is curettage, recurrence is infrequent.c. Langerhans Cell Histiocytosis: Swelling, pain,bleeding and loosening of teeth intraorally. Well defined periphery of the lesions radiographically, sometimes punched out appearance. The epicenter of bone destruction starts at midroot level as opposed to the periodontal lesions where the destruction starts at the crestal level. The mandible is more often involved than is the maxilla. It is found chiefly in the young, most patients are under the age of 30. The radiographic features are not diagnostic; biopsy is required for diagnosis. Chemotherapy is the mainstay of disseminated disease.
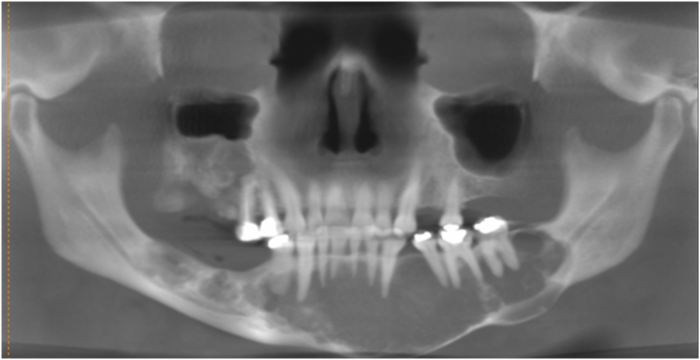
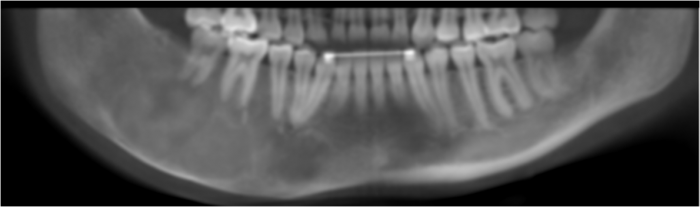
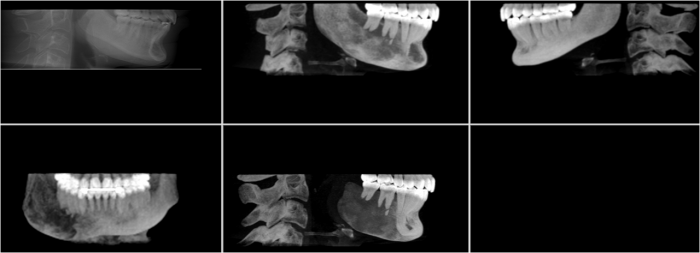
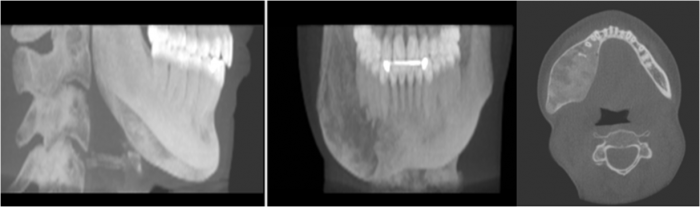
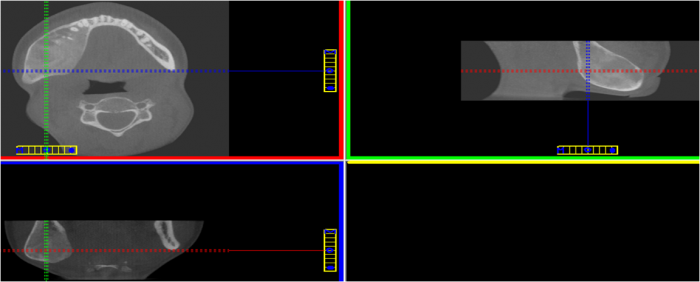
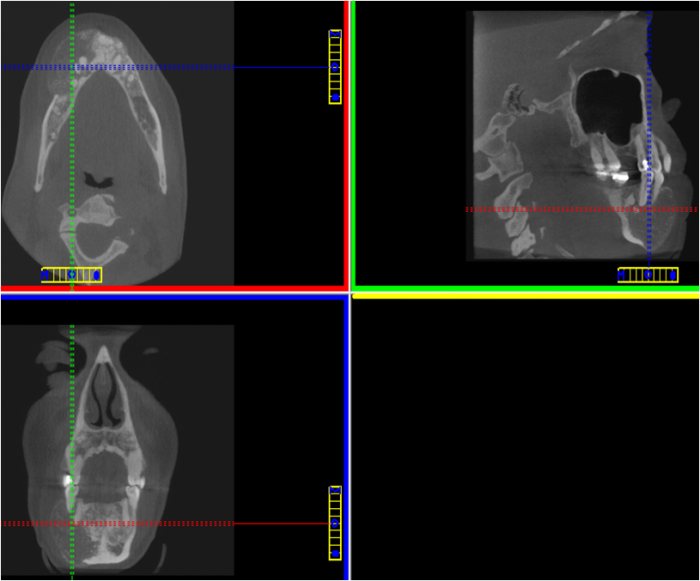
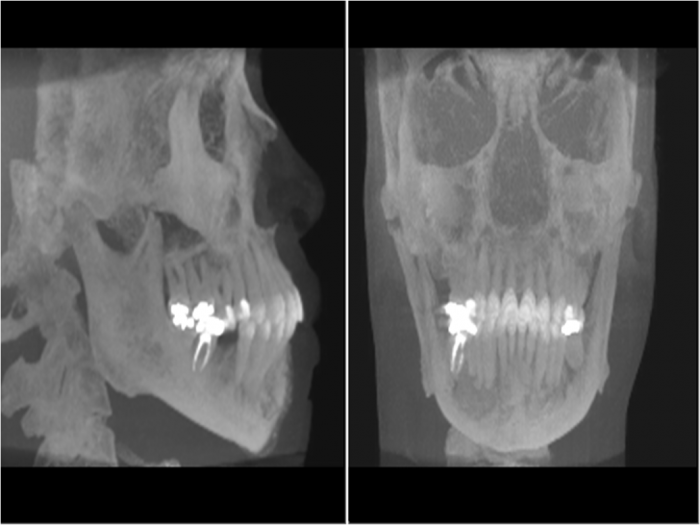
Florid cemento-osseous dysplasia
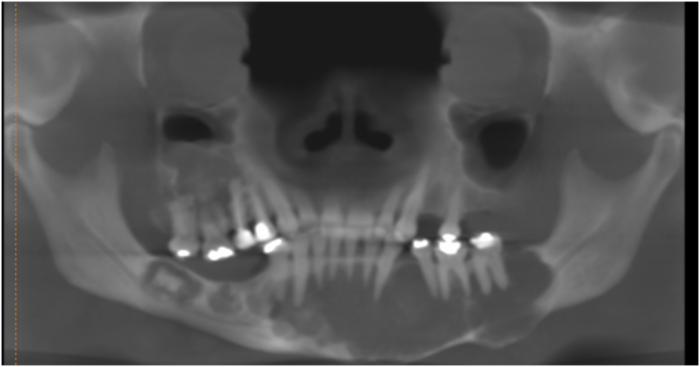
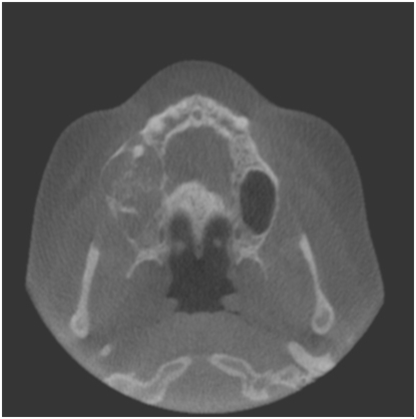
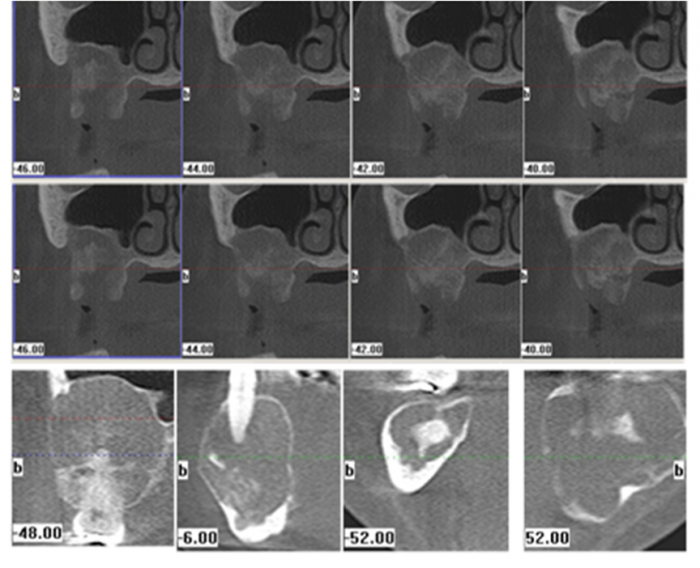
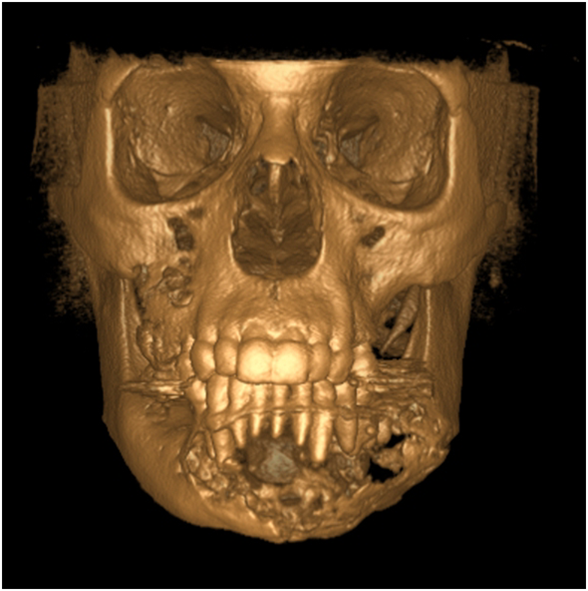
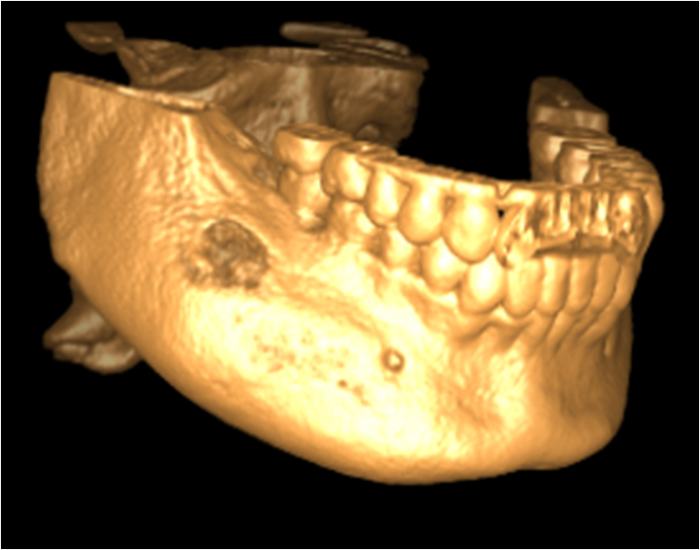
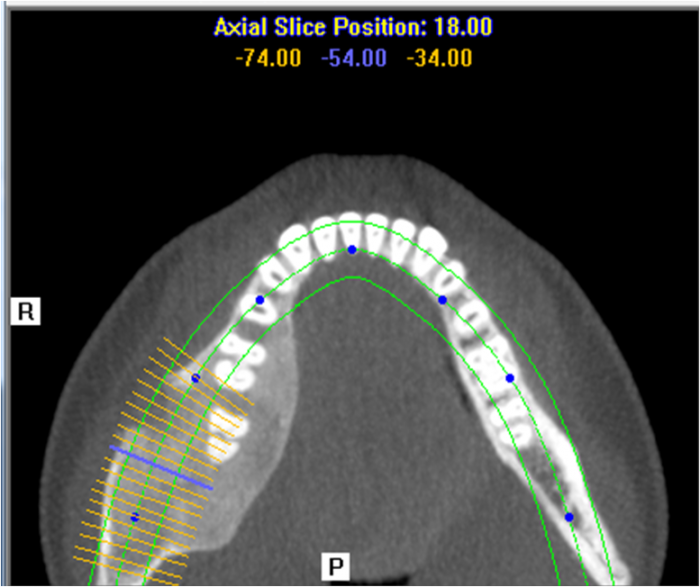
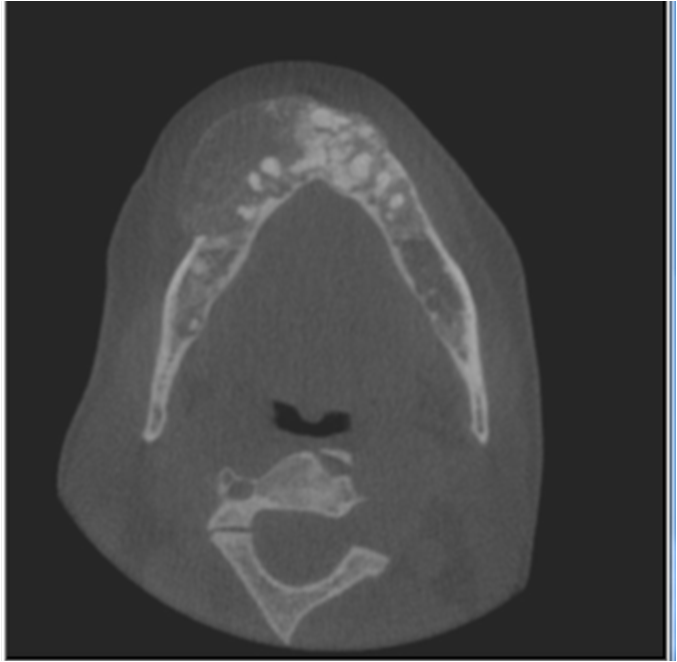
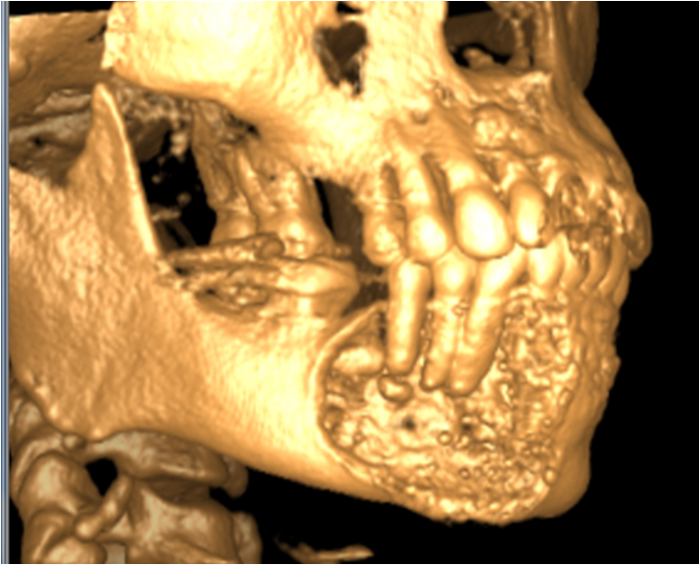
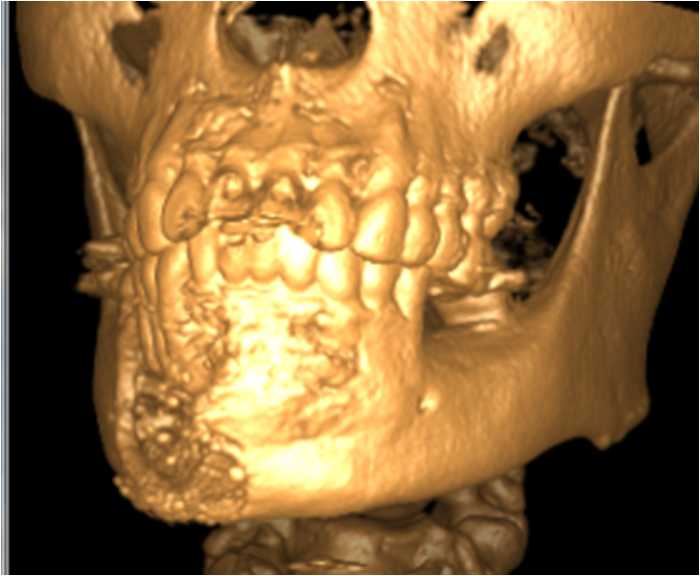
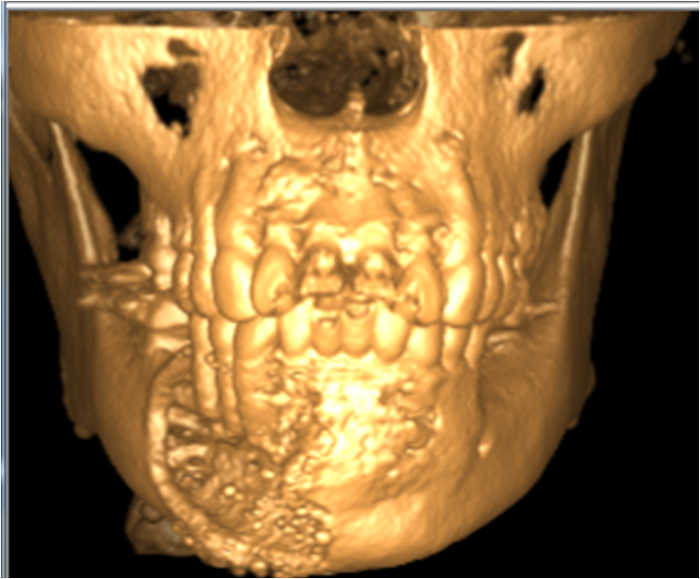
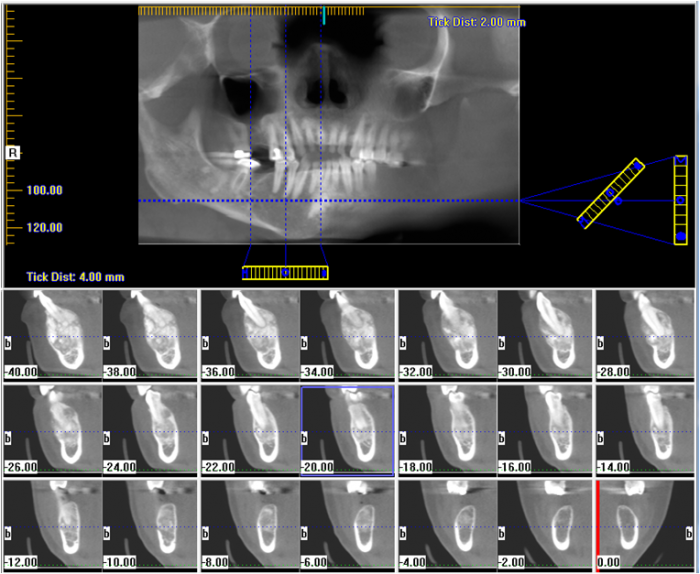
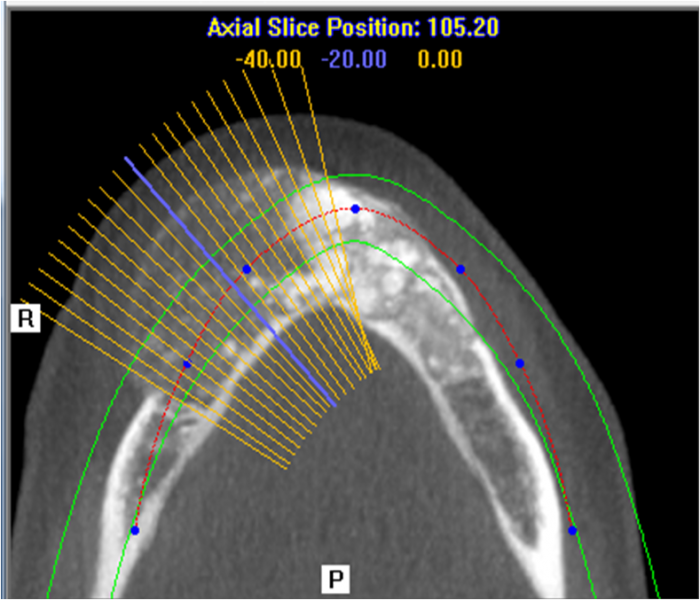
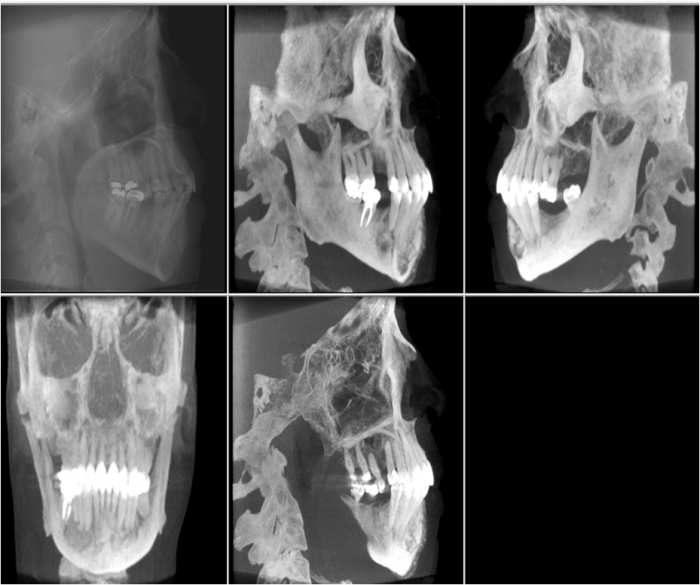
Fibrous Dysplasia
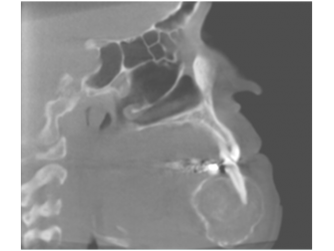
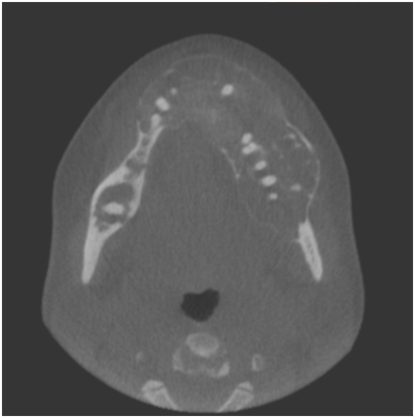
Ossifying Fibroma
khaled tarboush